Effect of rhPDGF-BB and Resorbable Barrier Membrane on Bone Regeneration in Three Dimensional Ridge Augmentation- A Clinical and Histomorphometric Study.
Hyung J. Kim, DDS, MSa, Kunal Lal, DDS, MSb
College of Dental Medicine, Columbia University; Columbia University Medical Center, New York, NY
Presented at the American College of Prosthodontics Annual Meeting table clinic presentation, Scottsdale, AZ, November 2008
a Former Resident, Postgraduate Prosthodontics, Columbia University CDM
b Assistant Clinical Professor, Postgraduate Prosthodontics, Columbia University CDM
Corresponding Author: Dr. Hyung J. Kim
28 Oak Street, Cresskill, NJ 07626
Phone: 201-693-3801, 82-55-542-2875 (Korea)
Fax:
E-Mail Address: hjk2113@columbia.edu, hjk348@yahoo.co.kr
Effect of rhPDGF-BB and Resorbable Barrier Membrane on Bone Regeneration in Three Dimensional Ridge Augmentation- A Clinical and Histomorphometric Study. Purpose: The primary purpose of this study was to evaluate the outcome of three-dimensional ridge augmentation in humans by combining rhPDGF-BB and anorganic bovine bone mineral. The secondary objective was to determine the value of a resorbable barrier membrane in combination with a titanium mesh when used with this tissue-engineered approach to bone regeneration. Material and Methods: In three patients with a combined horizontal and vertical bone deficiency, four therapeutic alveolar ridge augmentation procedures using following graft materials were conducted and evaluated. (1) Test-1: anorganic bovine bone mineral alone; (2) Test-2: anorganic bovine bone mineral saturated with rhPDGF-BB; (3) Test-3: A mixture of anorganic bovine bone mineral and synthetic beta-tricalcium phosphate (ß-TCP) saturated with rhPDGF-BB, covered with a titanium mesh; (4) Test-4: same as (3) but covered with a resorbable barrier membrane over a titanium mesh. After 6 months of healing period, biopsies were made and processed for histomorphometric analysis. Results: The healing was uneventful in all cases but in Test 3 with minor titanium mesh exposure. Histomorphometric analysis revealed that mean newly formed bone was 10%, 35%, 30%, and 20% for Test-1, Test-2, Test-3 and Test-4, respectively. The corresponding values for the residual graft material area parameter were 40%, 30%, 35%, and 35%. The fibrous tissue area was found to be 50%, 35%, 35%, and 45%, respectively. It appeared that considerably more new bone formation in quality and quantity was obtained in Test-2 and Test-3, compared with Test-1 and Test-4 therapeutic modalities. Conclusions: Within the limits of the present study, it can be concluded that rhPDGF-BB in humans played a considerable role in bone regeneration when used with anorganic bovine bone mineral, and placing a resorbable barrier membrane in combination with rhPDGF-BB appeared to adversely affect bone regeneration. Key words: Alveolar ridge augmentation, rhPDGF-BB, titanium mesh, resorbable membrane, tissue engineering, human study Introduction: Clinicians are frequently faced with the challenge of treating patients with significant bone loss resulting from periodontal disease, congenital abnormalities, tumors, traumatic injury, or resorption secondary to tooth loss. Successful implant therapy is dependent upon an adequate volume of bone at the site of implant placement, since the long-term prognosis of dental implants is adversely affected by inadequate bone volume.1
In principle, four methods have been described to increase the rate of bone formation and to augment bone volume: osteoinduction by the use of appropriate growth factors;2,3 osteoconduction, where a grafting material serves as a scaffold for new bone growth;4 distraction osteogenesis, by which a fracture is surgically induced and the two fragments are then slowly pulled apart;5 and finally, guided bone regeneration (GBR), which allows spaces maintained by barrier membranes to be filled with new bone.6,7 The guided bone regeneration technique implies that an enclosed space is created by the placement of a physical barrier, so that only bone-forming cells are allowed to populate the healing wound. Despite numerous studies have demonstrated successful outcomes of this treatment modality, vertical ridge augmentation has represented the most demanding indication in GBR therapy. The reported drawbacks of this approach to vertical ridge augmentation are donor site morbidity as well as its technical complexity, with frequent premature membrane (e-PTFE) exposure.8,9 In addition, the amount of vertical bone formation was not predictable and bone growth to the top of the membrane was not consistently reached when several millimeters of new bone formation were attempted. The remainder of the space between was occupied by non-mineralized tissue.10
Recent studies have demonstrated that growth factors can improve the capacity of alveolar bone to regenerate, improving cellular chemoattraction, differentiation, and proliferation.11,12 Platelet-derived growth factor (PDGF) has well-characterized, broad wound-healing activities in both hard tissue and soft tissue. Recently, purified recombinant human PDGF (rhPDGF) has been combined with allograft tissue or synthetic ceramic matrices such as beta-tricalcium phosphate (ß-TCP).13-15 Like most commercially available recombinant proteins, rhPDGF-BB (GEM 21S, BioMimetic Therapeutics) and rhBMP-2/ACS (INFUSE, Medtronic Sofamor Danek) are first produced by removing the specific DNA sequence from a human cell and transfecting it into a bacterial plasmid. The bacterial plasmid is then transfected into host cells capable of large-scale growth. In the case of rhPDGF-BB, the host cells are yeasts; in the case of rhBMP-2/ACS, the host cells are Chinese hamster ovary cells.11
Although a large-scale of randomized, controlled blinded clinical trial of the use of rhPDGF-BB to treat periodontal defects demonstrated rhPDGF-BB to be a potent stimulator of alveolar bone regeneration,16,17 the data available concerning the use of rhPDGF-BB in humans for three-dimensional alveolar bone augmentation in association with dental implants is lacking. In the present study, thus, it was primarily intended to evaluate the role of rhPDGF-BB in such situations.
To date, no conclusions have been drawn about the question whether or not bioactive molecules are best used in conjunction with membranes or in the absence of membranes.18,19 It is reasonable, on the one hand, to apply them as adjunctive agents to GBR therapy in order to accelerate membrane-guided bone regeneration. On the other hand, it may be hypothesized that their mode of action is best taken advantage of when membranes are not applied simultaneously, thus allowing all inducible cells from the wound environment access to the area to be regenerated. In view of this respect, the secondary purpose of this study was to determine the value of a resorbable barrier membrane in combination with a titanium mesh when used with this tissue-engineered approach to bone regeneration.
Materials and Methods
Study design:
In three patients with a combined vertical and horizontal bony deficiency in the anterior maxillae, four different therapeutic alveolar ridge augmentation procedures using following graft materials were conducted and evaluated clinically as well as in hostomorphometry. (1) Test-1: anorganic bovine bone mineral (Bio-oss) alone; (2) Test-2: anorganic bovine bone mineral saturated with rhPDGF-BB (GEM 21S); (3) Test-3: A mixture of anorganic bovine bone mineral (Bio-Oss) and synthetic beta-tricalcium phosphate (ß-TCP) saturated with rhPDGF-BB, covered with a titanium mesh; (4) Test-4: same as (3) but covered with a resorbable barrier membrane (BioMend-Extend) over a titanium mesh. All surgeries were carried out under local anesthesia. One hour before surgery the patients received antibiotics (Amoxicillin 500mg). For postoperative regimen, the patients were instructed to utilize an oral rinse of chlorhexidine (0.12%) twice daily for 10 days. Amoxicillin 500mg taken thrice daily for 5 days (or another appropriate antibiotic regimen) was also prescribed. After 6 months of healing period, biopsies were made and processed for histomorphometric analysis.
Clinical case descriptions:
All patients were healthy and non-smoking, with no systemic contraindication to intraoral surgery and implant placement. The patients agreed to participate in this study and provided written informed consent regarding grafting procedures and implant supported restorations.
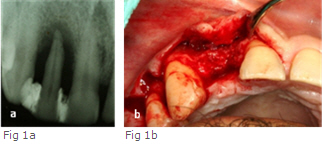
Patient 1 for Test-1: A 54 year old Hispanic male presented seeking for a tooth-supported fixed partial denture on extraction of the maxillary right lateral which was diagnosed a localized advanced periodontitis (Fig 1a). Periodontal probing depth measured 9mm and 8.5mm on the mesial and distal of the lateral incisor, respectively. In order to prevent an unaesthetic collapse of the alveolar ridge, pre-prosthodontic site development procedure was designed.20,21 The root of maxillary right lateral was eventually resected under the local anesthesia and the socket was thoroughly curetted to remove residual granulation tissue. Recipient site was perforated to expose the marrow spaces and encourage the bleeding. Anorganic bovine bone mineral (Bio-Oss, Osteohealth Co, Shirley, NY) alone in the absence of a barrier membrane was grafted. A sub-epithelial connective tissue pedicle graft was prepared from the palate to cover the graft and sutured with 5-0 polyglactine 910 (Vicryl; Johnson/ Ethicon). After uneventful healing period of 6 months, full-thickness mucoperiosteal flaps were elevated, and then a biopsy for the specimen of Test-1 was harvested from the ridge crest with a 2.7mm internal diameter trephine bur.
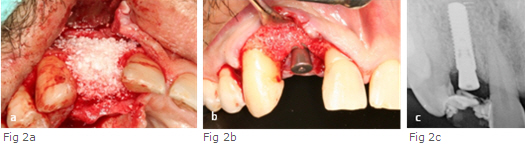
(2) Patient 1 for Test-2: The patient who initially sought for a tooth-supported fixed partial denture changed his mind into an implant restoration for the lateral incisor. Thus, all the particles of graft material which were incompletely integrated into native bone and embedded into the mucoperiosteal flaps were thoroughly eliminated. The recipient site was re-prepared in the same manner as in the Test-1. The Bio-Oss particles were saturated in the rhPDGF solution for 15 minutes as recommend by a manufacturer and grafted in the defect in the absence of a barrier membrane (Fig 2a). Extended sulcular incision with periosteal releasing incision encouraged tension-free primary closure of the mucoperiosteal flaps. After 6 months of healing period, the biopsy was harvested for the Test-2 specimen.
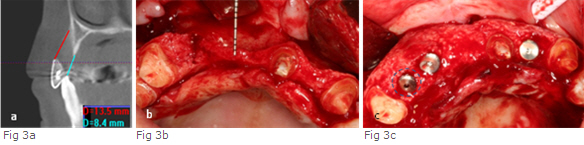
(3) Patient 2 for Test-3: A 56 year old Asian woman presented with the chief complaint of restoration of the non-salvageable upper right canine which had been engaged in an abutment of a six-unit ceramo-metal fixed partial denture. Upon clinical evaluation on the canine, thin attached gingiva (1mm) in combination with approximately 3mm gingival recession was present. In addition, interdental papilla was notably deficient on the mesial and distal. Probing depth measured 13 mm and 12mm on the mesial and distal of the canine, respectively. The sub-epithelial connective tissue (CT) graft was carried out on the labial gingiva at the same time the canine was extracted, to increase keratinized gingiva, preparing for an upcoming a three-dimensional bone augmentation. A CT scan obtained with a radiographic template in place revealed approximately 10mm and 5mm vertical bony deficiency on the labial and palatal of the defect at the right canine site (Fig 3a). Approximately 5mm horizontal bony deficiency with normal range of vertical height was measured at the site of left lateral incisor. After two months of soft tissue healing, the full-thickness mucoperiosteal flaps were elevated (Fig 3b). The recipient site was thoroughly debrided and perforated to open the marrow spaces. A mixture of Bio-Oss and ß-TCP saturated with rhPDGF-BB was grafted on the defect from the right canine to left lateral incisor. The titanium mesh (ACE dental co., N.J) which was shaped and adjusted earlier on the study model was secured with fixation screws on the labial surface of the alveolar ridge and tucked into the palatal flap to cover the graft. Periosteal releasing incision in combination with a palatal rotational pedicle connective tissue graft was carried out to allow for tension-free primary closure. After 6 months of healing, the specimen for the Test-3 was harvested at the site of canine.
(4) Patient 3 for Test-4: A 21 year old African woman presented with partial edentulism missing maxillary right lateral, central and left central incisor, in combination with severe alveolar ridge deficiency. Upon radiographic (CT scan) examination, it reveals an approximately 3mm-thick alveolar ridge with a vertical height deficiency (Fig 4a). The alveolar ridge augmentation procedure was performed in the same manner as in the Patient 2, except for an additional use of a resorbable membrane over the titanium mesh. After uneventful healing period of 6 months, a specimen for the Test-4 was harvested at the site of right lateral incisor.
Histologic preparation: The biopsy specimens were obtained with a 2.7mm internal diameter trephine bur and fixed in a solution of 10% buffered formalin for at least 48 hours at room temperature either with or without the trephine bur. They were then dehydrated in a graded series of alcohols (from 70% to 100%). They were decalcified overnight, then bisected and embedded in paraffin. The sections (4um) were made from paraffin-embedded specimen, then stained with hematoxylin and eosin (H&E) and mounted. The bone sections were observed with a light microscope equipped with a digital camera (Olympus BX41).
Results
Clinical evaluation
The healing was uneventful in all cases but in the Test-3, where minor titanium mesh exposure(approximately 7mm diameter) was noticed at 3 months of healing point. In this case, the patient was instructed to apply 0.12% chlorhexidine gel twice a day. Dental implants were successfully installed and restored in all patients.
In the Test-1: External topography of the ridge after the pre-prosthodontic site development procedure was well maintained until the reentry was made. Bio-Oss particles, however, embedded into the soft tissue were noticed when the flaps were elevated, and appeared to transform into fibrous tissue, which might result in thicker soft tissue. Bone regeneration appeared clinically incomplete in quantity as well as quality (Fig 1b).
In the Test-2: Mucoperiosteal flaps were clearly separated from the underlying regenerated bone with no difficulties, in contrast to the Test-1. No Bio-Oss particles embedded into soft tissue were noticed. The bone defect appeared to be completely filled with a hard tissue clinically resembling bone (Fig 2b). The vertical and horizontal bone gain was about 8mm and 5mm, respectively (Fig 2c, Table 2). An endosseous implant (Bone Level, NC 13mm, Straumann) was installed (Fig 2c) and restored at 6 months after.
In the Test-3: During the removal of the mesh, a thin layer of connective tissue was consistently observed underneath. This finding is consistent with a study of Boyne et al22 who described this layer as ‘‘pseudoperiosteum.’’ The bone defect appeared to be completely filled with a regenerated tissue clinically resembling bone. The vertical and horizontal bone gain was about 10mm and 8mm, respectively (Fig 3c, Table 2). Three implants (TiUnite, 4mm X 13mm, Nobel Biocare, Yorba Linda) were installed (Fig 3c). After 6 months of healing, a definitive restoration was delivered and a radiograph taken after a year revealed no active marginal bone resorption.
In the Test-4: While removing the titanium mesh, it appeared that fibrous tissue infiltrated through the coronal portion of the graft. The vertical and horizontal bone gain was about 1-2mm and 2-3mm, respectively (Fig 4b, Table 2). At 6 months, two implants (TiUnite, 3.3mm X 13m, 4.0mm X 13mm, Nobel Biocare, Yorba Linda) were installed on the site of right lateral and left central incisor (Fig 4c). Definitive restoration with pink porcelain on the cervical on the cervical was delivered to compensate the marginal bone loss.
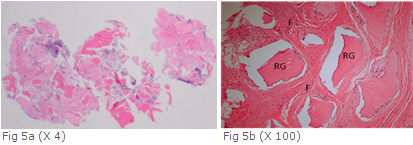
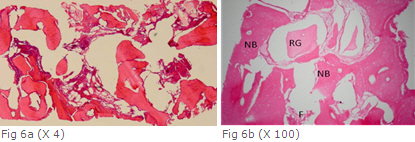
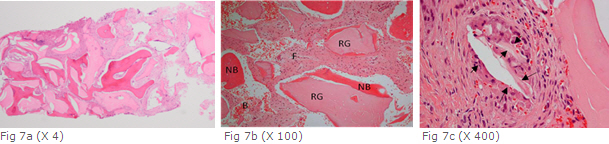
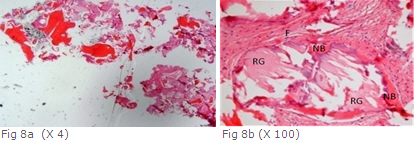
Histomorphometric Evaluation: The following parameters were measured on the specimens under the light miccroscope: percentage composition of newly formed bone (NF), fibrous tissue (F), and residual graft material (RG). In the Test-1 specimen, Bio-Oss particles on the coronal portion of the graft were completely surrounded by fibrous tissue (Fig 5a, 5b). In the Test-2 specimen, regenerated bone revealed a lamellar quality, characterized by a mature osteonic structure (Fig 6a, 6b). In the Test-3 specimen, eosinophilic homogenous acellular material consistent with residual graft material surrounded by osteoid in association with vascular fibrous tissue was noted (Fig 7a, 7b). In the Test-4 specimen, less formation of new viable bone (about 20%) is visible (Fig 8a, 8b). Histomorphometric analysis revealed that mean newly formed bone area was 10%, 35%, 30%, and 20% for the Test-1, Test-2, Test-3 and Test-4, respectively. The corresponding values for the residual graft material area parameter were 40%, 30%, 35%, and 35%. The fibrous tissue area parameter was found to be 50%, 35%, 35%, and 45%, respectively. It appeared that considerably more new bone formation was obtained in the Test-2 and Test-3, compared with the Test-1 and Test-4, while values for the fibrous tissue were opposite (Table 1).
Discussion
The present study demonstrated that the use of a growth factor, rhPDGF-BB in humans played a considerable role on inducing bone regeneration in the three-dimensional bone augmentation when used with anorganic bovine bone mineral (Bio-Oss). However, the use of resorbable barrier membrane (BioMend-Extend) in combination with the rhPDGF-BB appeared to adversely affect bone regeneration.
Autogenous bone has long been considered as the gold standard for bone regeneration procedures. It is thought to be osteocondcuctive and capable of providing vital osteogenic cells and signaling molecules. Autogenous bone harvesting, however, is invasive and presents with issues of morbidity. In this respect, a xenogenic graft, anorganic bovine bone mineral has been widely used as a bone substitute in implant dentistry23,24 and periodontology.25,26 In the present study (in the Test-2), rather than using synthetic beta-tricalcium phosphate (ß-TCP) included in the product (GEM 21S), anorganic bovine bone mineral (Bio-Oss) was used as a delivery vehicle of the growth factor, in order to meet the study design set. Anorganic bovine bone mineral has only osteoconductive properties27 which promote cellular adhesion and the formation of new bone tissue.
Since the biologic principles of guided tissue regeneration were applied by Nyman et al28 in the early 1980s, horizontal deficiencies such as fenestrations and/or dehiscence type defects around dental implants have been successfully treated. However, vertical ridge augmentation often requires the placement of autogenous, particulated or block bone grafts, or bone substitute materials in combination with e-PTFE membranes of various configuration.29,30 In vertical ridge augmentation, besides harvesting autogenous bone, the membrane exposure, resulting in bacterial contamination,8,9 is a phenomenon regularly reported in the literature, with exposure rates as high as 41% to 66%.31,32 Therefore, eliminating the need for the membrane and the autogenous bone harvesting would sensibly simplify and reduce the invasiveness of vertical ridge augmentation procedures. To overcome these problems which conventional GBR approach inherits, researchers and clinicians have been striving to develop less invasive surgical modalities that are less demanding technically and promote faster bone regeneration.
It is well known that growth factors are important to initiate and accelerate the normal processes involved in going from injury to repair.33 One signaling wound-healing molecule that has been extensively studied in preclinical models and humans is platelet-derived growth factor (PDGF), contained in the alpha granules of blood platelets and bone matrix34 and now recombinantly produced rhPDGF-BB for the treatment of periodontally related defects.35 Platelet-rich plasma (PRP) represents the first autologuous growth factor source available to dental and medical clinicians.36 First introduced by Marx et al. in 1998, it has been since demonstrated to be an effective osteopromoter in several standard bone regeneration techniques37,38 and osseointegration39,40 as well as a wound healing enhancer in numerous soft tissue applications.41 However, the benefit of using platelet rich plasma remains controversial. Currently, there is a lack of scientific evidence in the dental literature in favour of or against the clinical use of PRP for bone regeneration. In the study of Choi et al,42 to examine the effect of platelet-rich plasma on bone regeneration in an autogenous bone graft, continuity resection was performed on both sides of the mandible in a canine model. The histologic analysis of the biopsies after 6 weeks revealed lower levels of bone formation in the PRP group than in the non-PRP group, and fluorescence microscopy revealed a delay in the remodeling of grafts loaded with PRP. They speculated that the explanation with the results is related to the concentration of PRP within the bone graft. Variations in the concentration of platelet-derived growth factor (PDGF) are known to influence bone healing.43-45
In the present study, it was intended to test the potential of the rhPDGF-BB by placing Bio-Oss alone in the Test-1 and Bio-Oss saturated with rhPDGF-BB in the Test-2 in the absence of the barrier membrane at the same site of the patient. It is known that the purified recombinant human PDGF (rhPDGF) provides approximately 1,000 times greater concentration of PDGF than that which is commonly obtained through platelet concentration.46,47 Thus, evidence of beneficial effects of rhPDGF-BB in the present study may be drawn to difference of the concentration of the growth factor.33-35
In the study of Zechner et al48 in 2003, histologic evaluation in minipigs showed significant more bone-to-implant contact after topical PRP application in the early healing phase (6weeks), which varied as a function of the distance from the implant surface (controls=24.2% versus PRP=44.21%; P=.013) at 12 weeks, the extent of osteogenesis was comparable in the 2 groups (controls=51.3% versus PRP=44.2%; P=.251). They demonstrated that topical application of PRP significantly increase the activity of bone regeneration at implant host sites during early healing and concluded PRP has time- and site dependent effect on peri-implant bone healing. In view of these results, the morphology of the defect at the site of bone regeneration has a significant impact on the result of treatment with PRP. In the combined vertical and horizontal defect as much as in the present study, early healing of ridge augmentation can be of paramount importance for successful bone regeneration because it has much more possibility to be influenced by micromovements which can cause fibrous repair. In contrast, in situations with the sinus elevation procedures, the reported effects of PRP (compared with their controls) are considered to be weak.49,50
Besides ample vascular supply to the graft, mechanical rest is a prerequisite for graft integration and bone regeneration.51 Von Arx et al52 in 1999 demonstrated that using the titanium mesh can prevent barrier collapse. Furthermore, micromovements hindering proper vertical bone regeneration are more likely to occur in sites covered with non-reinforced membranes than in sites treated with a titanium mesh. Exposure of the titanium mesh at 3 months was observed in the Test-3 in the present study. This is a common phenomenon when titanium mesh is used for ridge augmentation. For example, von Arx et al experienced exposure of the mesh in 50% of their cases. Despite the exposure, no infection was noticed in any of the patients.
The secondary objective of the present study was to determine the value of a resorbable barrier membrane when used with this tissue-engineered approach to bone regeneration. The benefit of using both barrier membranes and growth factors/differentiation factors for bone augmentation has been debatable.18,19 Cochran et al53 in 1997 reported that the presence of a non-resorbable e-PTFE membrane initially (4 weeks) inhibited bone formation with rhBMP-2 but did no longer do so at later time points (12 weeks). It has been shown that bone induction by rhBMP-2 occurs at early time points and that rhBMP-2 undergoes rapid clearance. Hence, the use of a membrane may potentially reduce the bone-forming effect of rhBMP-2 due to limited availability of inducible cells. Another animal study in rats reported no difference in bone healing with the combination of rhBMP-2 and an e-PTFE membrane compared to rhBMP-2 alone.54 From a clinical point of view, the use of a membrane simplifies the handling and stabilization of bone substitute mineral at the time of bone augmentation, but from a biologic point of view the use of a membrane may block the recruitment of cells from the environment.
Recently reported studies by Simion et al. in a dog model with a three dimensional bone augmentation procedure12 (in 2007) demonstrated that clearly important are the superior results obtained with the addition of rhPDGF-BB (GEM 21S) but without placement of an overlying collagen barrier membrane. In this study, the group which used a deproteinized bovine block saturated with rhPDGF-BB in the absence of a barrier membrane showed a significant amount of new bone formation, particularly at the coronal portion of the regenerated tissue facing the periosteum and the soft tissues. The result in the present study in humans is consistent with their study in that less amount of bone regeneration was observed where a resorbable barrier membrane was placed to a tissue-engineered approach. Unlike traditional GBR procedures, where placement of an appropriate barrier membrane is integral to the success of the procedure, the growth factor-mediated regeneration method examined in the present study suggests that barrier membranes are not only not required (in the Test-2, Test-3), but may prevent an adequate regenerative response (in the Test-4). It must be mentioned, however, that the lack of increased bone regeneration in response to rhPDGF-BB in the Test-4 may be due to smaller number of osteogenic cells from the medulla of very thin alveolar ridge capable of responding to rhPDGF-BB. Nevertheless, the results in the present study implies that the use of synthetic materials in the absence of the barrier membrane would result in lower surgical risks and lower morbidity in the augmentation procedure and would represent an important step forward in simplifying bone regeneration procedures.
Conclusion
Within the limits of the present study, it can be concluded that rhPDGF-BB in humans played a considerable role on bone regeneration in the three-dimensional bone augmentation, and placing a resorbable barrier membrane in combination with rhPDGF-BB may adversely affect bone regeneration. Further studies with the randomized controlled trials are needed that will assess the role of this rhPDGF-BB and the value of a resorbable barrier membrane when used with this tissue-engineered approach to bone regeneration.
Acknowledgment
The authors gratefully acknowledge a professor of oral pathology, Angela J. Yoon for histologic processing and her advice, and a clinical assistant professor, Dr. Spicer for his passionate educational support.
References
Lekholm U, Adell R, Lindhe J, et al. Marginal tissue reactions at osseointegrated titanium fixtures. A cross-sectional retrospective study. Int J Oral Maxillofac Surg 1986;15:53-61.
Urist MR. Bone: Formation by autoinduction. Science 1965;150:893-899.
Reddi AH. Role of morphogenic proteins in skeletal tissue engineering and regeneration. Nat Biotechnol 1998;16:247-252.
Buch F, Albrektsson T, Herbst E. The bone growth chamber for quantification of electrically induced osteogenesis. Journal of Orthopedic Research 1986;4:194-203.
Ilizarov GA. The tension-stress effect on the genesis and growth of tissues: Part II. The influence of the rate and frequency of distraction. Clinical Orthopedics 1989;239:263-285.
Dahlin C, Linde A, Gottlow J, Nyman S. Healing of bone defects by guided tissue regeneration. Plastic and Reconstructive Surgery 1988;81:672-677.
Nyman SR, Lang NP. Guided tissue regenerationand dental implants. Periodontology 2000;4:109-118.
Simion M, Trisi P, Piattelli A. Vertical ridge augmentation using a membrane technique associated with osseointegrated implants. Int J Periodontics Restorative Dent 1994;14:496-511.
Simion M, Trisi P, Maglione M, Piattelli A. Bacterial contamination in vitro through GTAM membrane with and without topical chlorhexidine application. A light and scanning electron microscopic study. J Clin Periodontol 1995;22:321-331.
Simion M, Trisi P, Piattelli A. vertical ridge augmentation using a membrane technique associated with osseointegrated implants. International Journal of Periodontics and Restorative Dentistry 1994b;14:497-511.
Lynch SE, Marx RE, Nevins M et al. 2nd ed; Tissue Engineering: Application in Oral and Maxillofacial Surgery and Periodontics. Quintessence Publishing 2008;47-63.
Simion M, Dahlin C, Rocchietta I, Stavropoulos A, Sanchez R, Karring T. vertical ridge augmentation with guided bone regeneration n in association with dental implants: An experimental study in dogs. Clin Oral Implants Res 2007;18:86-94.
Lynch SE. Bone regeneration techniques in the orofacial region. In: Lieberman J, Friedlaender G (eds). Bone Regeneration and Repair: Biology and Clinical Applications. Totowa, NJ: Humana Press 2005:359-390.
Nevins M, Camelo M, Nevins ML, Schenk RK, Lynch SE. Periodontal regeneration in humans using recombinant human platelet-derived growth factor BB (rhPDGF-BB) and allogenic bone. J Periodontol 2003;74:1282-1292.
Leslie A, Wisner-Lynch. From passive to active: Will recombinant growth factor therapeutics revolutionize regeneration? The International Journal of Periodontics & Restorative Dentistry 2006;26:409-411.
Nevins M, Giannobile WV, Mc Guire MK, et al. Platelet-derived growth factor stimulates bone fill and rate of attachment level gain: Results of a large multicenter randomized controlled trial. J Periodontol 2005;76:2205-2215.
McGuire MK, Kao RT, Nevins M, Lynch SE. rhPDGF-BB promotes healing of periodontal defects: 24-month clinical and radiographic observations. Int J Periodontics Restorative Dent 2006;26:223-231.
Howell TH, Fioreellini JP, Jones A, Alder M. et al. A feasibility study evaluating rhBMP-2/absorbable collagen sponge device for local alveolar ridge preservation or augmentation. International Journal of Periodontics and Restorative Dentistry 1997;17:125-139.
Jung RE, Glauser R, Scharer P, Hammerle CHF, Weber FE. The effect of rhBMP-2 on guided bone regeneration in humans. A randomized, controlled clinical and histomorphometric study. Clinical Oral Implants Research 2003;14:556-568.
Bahat O, Deeb C, Komarnyckyi O. Preservation of ridge utilizing hydroxyapatite. Int Periodontol Rest Dent 1987;6:35-41.
Cohen ES. Ridge Enhancement and Socket Preservation Utilizing the Subepithelial Connective Graft: A case report. Pract Periodont & Aesthet Dent 1995;7:53-58.
Boyne PJ, Cole MD, Stringer D. Shafqat JP. A technique for osseous restoration of deficient edentulous maxillary ridges. Journal of Oral and Maxillofacial Surgery 1985;43: 87-91.
Zitzmann NU, Scharer P, Marinello CP. Long-term results of implants treated with guided bone regeneration: A 5-year prospective study. Int J Oral Maxillofac Implant 2001;16:355-366.
Hammerle CH, Lang NP. Single stage surgery combining transmucosal implant placement with guided bone regeneration and bioresorbable materials. Clin Oral Implants Res 2001;12:9-18.
Camelo M, Nevins ML, Schenk RK, et al. Clinical, radiographic, and histologic evaluation of human periodontal defects treated with Bio-Oss and Bio-Gide. Int J Periodontics Restorative Dent 1998;18:321-331.
Camelo M, Nevins ML, Lynch SE, Schenk RK, Simion M, Nevins M. periodontal regeneration with an autogenous bone-Bio-Oss composite graft and a Bio-Gide membrane. Int J Periodontics Restorative Dent 2001;21:109-119.
Hammerle CH, Karring T. Guided bone regeneration at oral implant sites. Peiodontol 2000 1998;17:151-175.
Nyman S, Karring T, Lindhe J, Planten S. Healing following implantation of periodontitis-affected roots into gingival connective tissue. J Clin Periodontol 1980;7:394-401.
Simion M, Baldoni M, Rossi P, Zaffe D. A comparative study of the effectiveness of e-PTFE membranes with and without early exposure during the healing period. International Journal of Periodontics and Restorative Dentistry 1994a;14:167-180.
Tinti C, Parma-benfenati S. Vertical ridge augmentation: surgical protocol and retrospective evaluation of 48 consecutively inserted implants. International Journal of Periodontics and Restorative Dentistry 1998;18:445-443.
Becker W, Becker BE, McGuire MK. Localized ridge augmentation using absorbable pins and ePTFE membranes: A new surgical approach. International Journal of Periodontics and Restorative Dentistry 1994;14:48-61.
Zitzmann NU, Naef R, Scharer P. Resorbable vesus non-resorbable membranes in combination with Bio-Oss fro guided bone regeneration. Int J Oral Maxillofac Implant 1997;12:844-852.
Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85(6):638-646.
Lynch SE. Introduction. In: Lynch SE, Genco RJ, Marx RE (eds). Tissue Engineering: Applications in Maxillofacial Surgery and Periodontics, ed I. Chicago: Qintessence, 1999:xi-xviii.
Nevins M, Giannobile WV, McGuire MK, et al. Platelet-derived growth factor stimulates bone fill and rate of attachment level gain: Results of a large multicenter randomized controlled trial. J Periodontol 2005;76:2205-2215.
Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85: 638-646.
Kassolis JD, Rosen PS, Reynolds MA. Alveolar ridge and sinus augmentation utilizing platelet-rich plasma in combination with freeze -dried bone allografts. Case series. J Periodontol 200;71:1654-1661.
Carmargo PM, Lekovic V, Weinlaender M, Vasilic N, Madzarevic M, Kenney EB. Platelet-rich plasma and bovine bone mineral combined with guided tissue regeneration in the treatment of infrabony defects in humans. J periodontal Res 2002;37:300-306.
Rodriguez A, Anastassov GE, Lee H, Buchbinder D, William H, Maxillary sinus augmentation with deproteinated bovine bone and platelet rich plasma with simultaneous insertion of endosseous implants. J Oral Maxillofac Surg 2003;61:157-163.
Marx RE, Garg AD. Dental and craniofacial applications of platelet-rich plasma. Chicago: Quintessence, 2005.
Jackson RF. Using platelet rich plasma to promote healing and prevent seroma formation in abdominoplasty procedures. Am J Cosmet Surg 2003;20:187-192.
Choi BH, Im CJ, Huh JY, Suh JJ, Lee SH. Effect of platelet-rich plasma on bone regeneration in autogenous bone graft Int. J. Oral Maxillofac. Surg 2004;33: 56-59.
Lee MB. Bone morphogenetic proteins: Background and implications for oral reconstruction. A review. J Clin Periodontol 1997;24: 355-365.
Marden L, Fan R, Pierce G, Reddi A, Hollinger J. Platelet-derived growth factor inhibits bone regeneration induced by osteogenin, a bone morphogenic protein, in rat craniotomy defects. J Clin Invest 1993;92:2897-2905.
Sutherland D, Bostrom M. Grafts and bone graft substitutes. In: Lieberman JR, Friedlaender GE (eds). Bone Regeneration and Repair Biology and Clinical Applications. Totowa, NJ: Humana, 2005:133-156.
Huang JS, Huang SS, Deuel TF. Human platelet-derived growth factor in vivo: Levels, activity, and discovery of a specific plasma-binding protein. J Cell Biol 1983;97:383-388.
Harvest Technologies Corporation. Bioactive Proteins-Faster Healing. Available at: http://www.harvesttech.com/education/ intro.html. Accessed 23 Jun 2010.
Zechner W, Tangl S, Tepper G, FúRst G, Bernhart T et al. Influence of Platelet-rich Plasma on Osseous Healing of Dental Implants: A Histologic and Histomorphometric Study in Minipigs. Int J Oral Maxillofac Implants 2003;18:15-22.
Adelina S. Plachokovan Dimitris Nikolidakisn Jan Mulder John A. Jansen Nico H. J. Creugers Effect of platelet-rich plasma on bone regeneration in dentistry: a systematic review Clin. Oral Impl Res 2008;19:539-545.
Froum SJ, Wallace SS, Tarnow DP, Cho SC. Effect of Platelet-Rich Plasma on Bone Growth and Osseointegration in Human Maxillary Sinus Grafts: Three Bilateral Case Reports. The International Journal of Periodontics & Restorative Dentistry 2002;22:45-53.
Oh TJ, Meraw SJ, Lee EJ, Giannobile WV, Wang HL. Comparative analysis of collagen membranes for the treatment of implant dehiscence defects. Clinical Oral Implants Research 2003;14:80-90.
von Arx T, Kurt B. Implant placement and simultaneous ridge augmentation using autogenous bone and a micro titanium mesh: a prospective clinical study with 20 implants. Clin Oral Impl Res 1999;10:24-33.
Cochran DL, Nummikoski PV, Jones AA, Makins SR, Turek TJ, Buser D. Radiographic analysis of regenerated bone around endosseous implants in the canine using recombinant human morphogenic protein-2. Int J Oral Maxillofac Implants 1997;12:739-748.
Linde A, Hedner E. Recombinant bone morphogenic protein-2 enhances bone healing, guided by osteopromotive e-PTFE membranes: An experimental study in rats. Calcified Tissue International 1995;56:549-553.
Illustrations and Tables
(1) Test-1
(2) Test-2
(3) Test-3
(4) Test-4
Photomicrographs
(1) Test-1
(2) Test-2
(3) Test-3
(4) Test-4
Tables
Table 1. Summary of the histomorphometric analysis
Table 2. Outcomes after four different ridge augmentation procedures
위의 연구 논문은 “Intrernational Journal of Oral Maxillofacial Implant (IJOMI)" 라는 치과계 최고 권위의 임플란트 학술저널에 곧 게제될 논문으로 치조골 재건 시술에 있어 성장호르몬의 하나인 rhPDGF-BB 와 Barrier membrane 의 역할이라는 주제입니다.

![진료시간안내 [평일]09:30 ~ 19:00, [토요일]09:30 ~ 14:00, [수요일]09:30 ~ 21:00, 공휴일/일요일 휴무](/images/sub_left_banner02.gif)